Penny, a Norfolk and Suffolk NHS Foundation Trust (NSFT) carer, spoke on behalf of our campaign at the Norfolk Health Overview and Scrutiny Committee (HOSC) of Norfolk County Council today:
Thank you for the opportunity of addressing you on behalf of the Campaign about issues arising from the Verita report. I am the nearest relative of a service user with ten years of involvement with NSFT and for a short time I was an assistant deputy coroner.
I would like to make two main points:
- the terms of reference of the Verita report;
- the validity of the data.
Relating to the terms of reference
The terms of reference of the report appear on page six and also at Appendix A. Most relate to policy, processes and compliance with criteria. Almost as an aside the very last sentence of the terms of reference invites consideration of this question : “Are there trends that indicate concerns in specific locations or services?”
If you go to Verita’s own website you will see that Verita offers a serious incident diagnostic tool which tests the effectiveness of SI investigation against seven best practice standards. The fourth test is against resource and infrastructure. The nearest the terms of reference came to this was the aforementioned investigation into locations and services. Noting that, I could not find anything in Verita’s analysis or recommendations which did even that. So the report has not addressed the possibility that the increasing death rate (whether or not in line with national averages) is in any way related to the availability of resources and the delivery or otherwise of services. We believe that is a serious omission.
The Campaign suggests Verita should have been tasked to interrogate whether the radical redesign and the reduction of services has had an impact on the mortality figures. This Campaign started in 2013 as a result of NSFT staff having unresolved concerns about a cluster of deaths following the radical redesign and the cuts to services and lack of available beds. It continues to have those concerns and this report, good though it is, does not assuage those concerns.
The questions we should be asking: whether the NSFT is properly resourced and the infrastructure appropriate to prevent (so far as is possible) unexpected patient deaths; not whether NSFT have followed the appropriate processes. These vital questions remain unanswered despite the Verita report.
The report looks into unexpected patient deaths. But what about those people who died suffering from mental illness who were not patients? For example, those street sleepers who have been unable to get support because of the disbandment of the Homeless Team and the Assertive Outreach Team. Sadly, if you are not already a service user, i.e. in the system, access to timely support in a crisis is left to the Samaritans, A&E or the Police. Access to services must be a relevant factor in preventing suicides and unexpected deaths.
The validity of data.
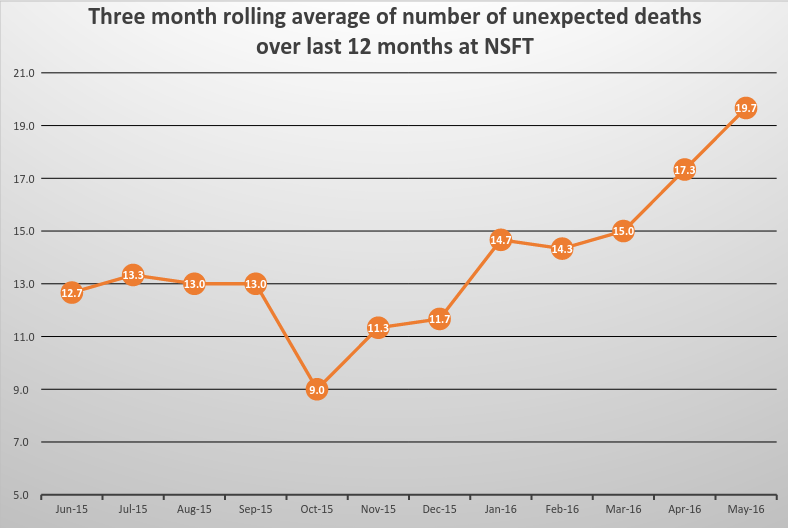
Data can be incomplete and sometimes wrong or taken out of context but the Campaign submitted the graph (Appendix D) based on figures supplied by NSFT [see below].
At the bottom is a note added to our document at the request of NSFT so I would like to comment on that. Is it the case then that for the period April 2015 to February 2016 all those figures have been arrived at after an Inquest or the investigation is complete? We think not, natural causes may have been included in the pre March 2016 figures as well as the post March ones. We have never known provisional figures given before, so why are the post March figures supplied to us by the Trust now provisional? All the figures in the graph have been supplied to us by the Trust without distinction that is until we compiled them into a graph for submission today .
But it is not just this year and last year. In 2012-13 there were 88 unexpected deaths i.e about 7 (7.3 to be exact) per month whereas in the first two months of this year there were 21 deaths per month. In the last three years the number has tripled. The Campaign asks the question “Why” and invites the Committee to scrutinise these figures further.
Interrogating/scrutinising this data is very important. Conscious of time constraints and the scope of my representation to you I mention briefly Reports to Prevent Future Deaths. These arise following a Coroner’s Inquest where the Coroner believes action should be taken to prevent future deaths. S/he has a duty to make a report to the responsible organisation (formerly called Rule 43 reports). A retired NHS consultant psychiatrist (Dr Alexander) did some painstaking work and reported to the Health Select Committee in June of this year with the results of her analysis of the 379 most notable of these Reports from July 2008 to June 2016. Norfolk and Suffolk NHS Foundation Trust was sent 22 reports which is the highest number of warning reports to any trust in England. We can supply Dr Alexander’s research to the Committee if this would be helpful .
Why so many unexpected and increasing NSFT patient deaths year on year and why so many Coroner’s warning reports? We urge the Committee to scrutinise this further.