
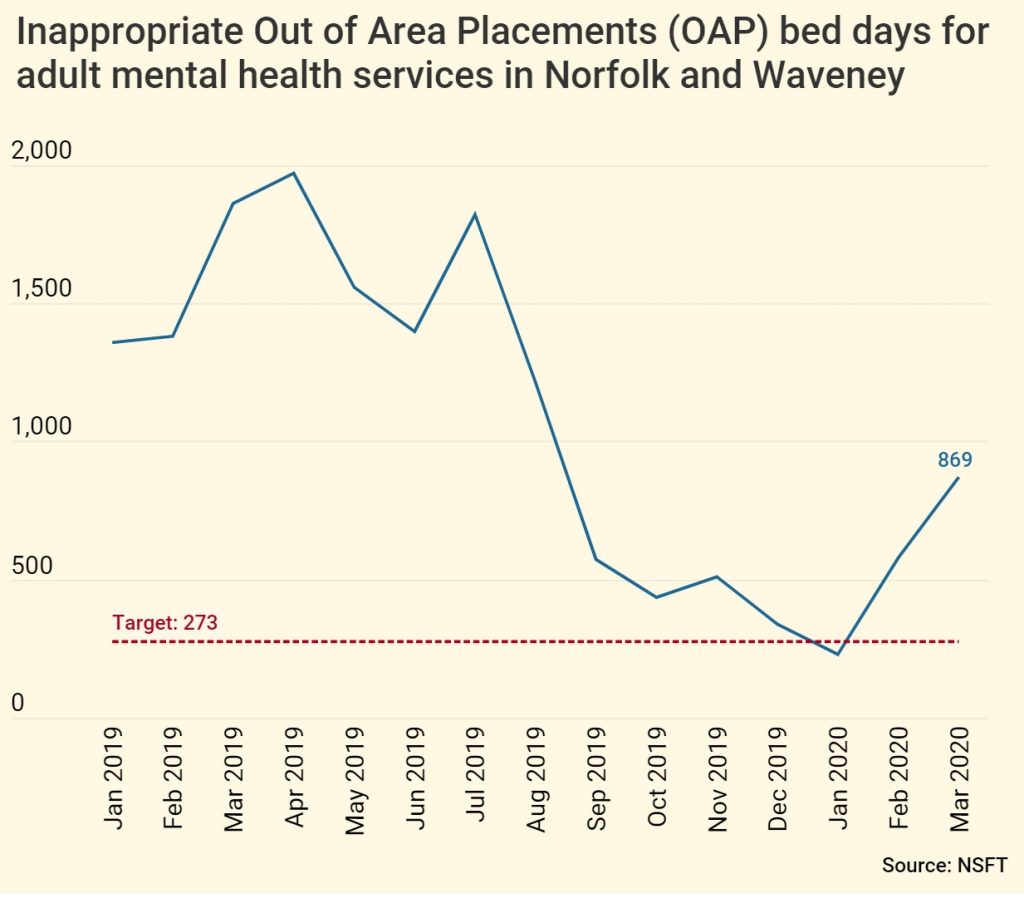
It has long been clear that Norfolk & Suffolk NHS Foundation Trust (NSFT) tries to manipulate its inappropriate out of area placement (OAP) bed statistics when the Care Quality Commission (CQC) comes to inspect. As the graph below shows, out of area bed usage was again artificially reduced in the run-up to the latest full CQC inspection during October 2019, only to rise again shortly thereafter, even following NSFT’s blatant attempt to fiddle the most recent figures by excluding £560 per night beds at the remote private hospital on the site of the repeatedly-inadequate Mundesley Hospital which was forced to close by CQC, Southern Hills, on the basis that these placements are not inappropriate since a manager from NSFT visits the site twice per week:
There is a bed crisis because NSFT closed at least 139 of its mental health beds at the same time as its community mental health services were slashed and specialist services were closed. NSFT has recently reopened sixteen beds but these are nowhere near enough to address the beds crisis, particularly when community services remain chronically underfunded. NSFT’s Board and senior management consistently finds the money for new management posts, promotions and pay rises for themselves, relatives and friends but doesn’t seem to care about the quality of mental health services received by the people of Norfolk and Suffolk.
Now, whistle-blowers have provided us with the latest so-called ‘Bed Management Escalation Process’ for central Norfolk, the heart of the beds crisis under the so-called ‘leadership’ of Andy Mack, the brother of the so-called ‘manager’ of repeatedly-inadequate mental health services for Children, Families and Young People (CFYP), Rob Mack. Between them, this particular band of brothers is trousering more than £150,000 per annum from NHS coffers. We and many front line staff have no confidence in either of them. They should be sacked without compensation. You can bet the manager pretending to be Clinical Director, Claire Lussignea, will have been utterly ineffective in representing clinicians and patients in the formulation of this process because ineffective is what she has been ever since she played a central role in the radical redesign disaster.
The ‘Bed Management Escalation Process’ shows how, once mental health professionals have made the clinical decision that a person needs an admission to hospital, trust managers put bureaucratic barriers and delays in the way to stall and prevent admissions; how people are treated differently when no trust bed is available; and how bureaucratic targets override clinical priorities. And this after the delays we know the lack of beds causes to the section assessment process, as Approved Mental Health Professionals (AMHPs) are understandably loathe to arrange Mental Health Act assessments in the absence of available beds: section papers cannot be legally completed without the destination hospital being named and AMHPs are supposed to stay with patients and families until a bed is found, which can take days. CTO recalls often take days and have sometimes taken many weeks.
Here is what is supposed to happen in the fortunate event that there is a bed available at NSFT:
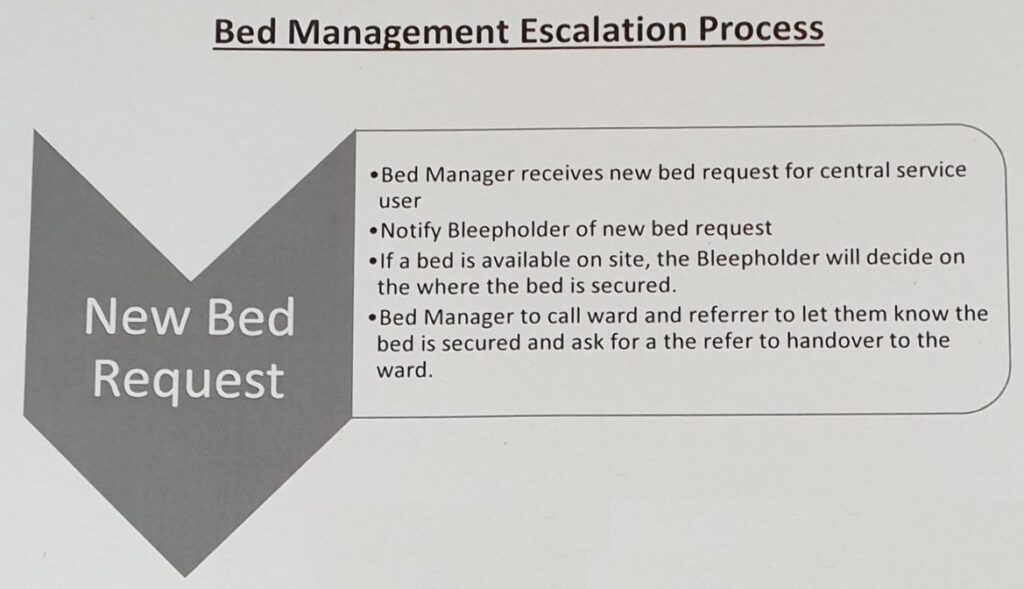
This is pretty much what would be expected. We’re reasonably happy with this: it is what should happen every time because NSFT should have enough beds of its own. So far, two managers are involved who haven’t met the patient (Bed Manager and Bleepholder).
But what happens if there isn’t a bed at central services, i.e. Hellesdon Hospital?
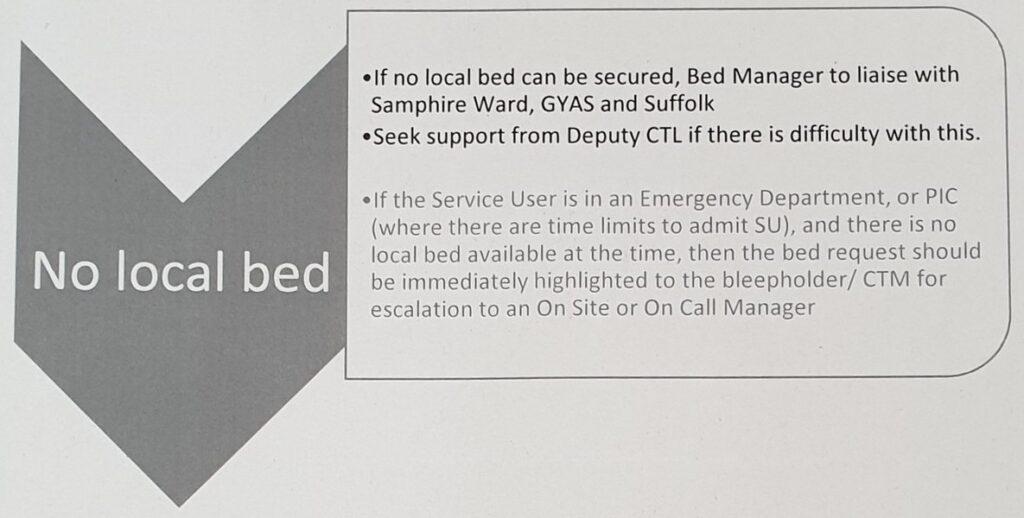
If there is no local bed, NSFT managers will try to find a bed in King’s Lynn, Great Yarmouth or Suffolk. We know that many people in Suffolk and North East Essex believe that their beds should not be used to hide the lack of beds commissioned by Norfolk & Waveney – in fact, Suffolk would replace NSFT as its provider if it could.
None of these distant solutions are acceptable to us, as the beds are not local and should not be routinely used, but they are. Yet another manager will be involved if there are problems. There are now at least three managers who haven’t met the patient involved (Bed Manager, Deputy CTL and Bleepholder/CTM) but not enough beds.
But, if the person in need of admission is in an environment which has a target attached to it, such as Accident & Emergency or in a police cell (PIC), they receive preferential treatment not because of clinical need but to fiddle the figures as the bed request is escalated to yet another manager. There are now at least four managers who haven’t met the patient involved (Bed Manager, Deputy CTL, Bleepholder/CTM and On site/call Manager) but still no bed.
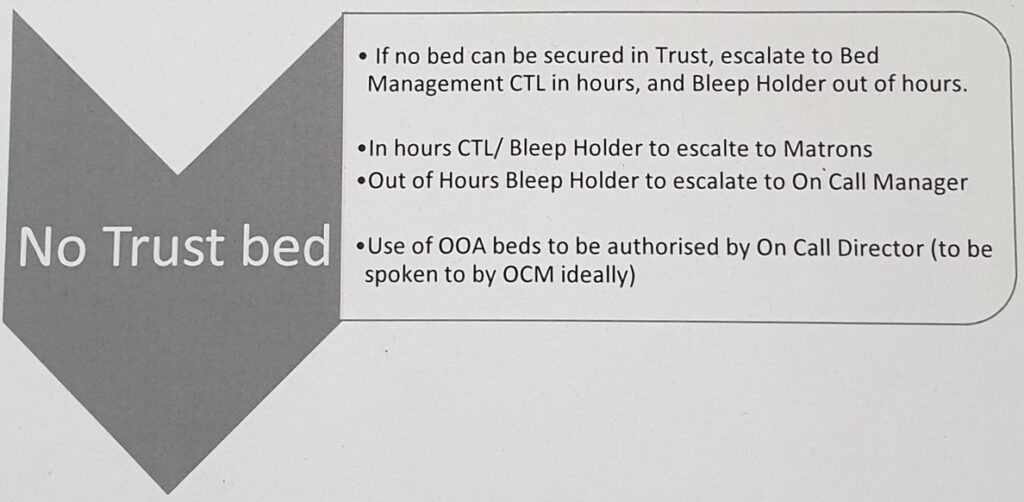
After hours of delay and confirmation that there is no bed available, the issue will be escalated to the CTL/Bleepholder, Matrons/on Call Managers.
If they can’t pressure clinicians to discharge somebody else who wasn’t going to be discharged, sometimes homeless or to some random Bed & Breakfast miles away from their home and community mental health team, frequently very ill and with little to no discharge planning, to empty a bed for the new admission, they will eventually call an On Call Director to authorise the use of an Out of Area bed.
There are now at least five managers who haven’t met the patient involved (Bed Manager, Deputy CTL, Bleepholder/CTM, On site/call Manager and On Call Director) but still no bed. What do any of these managers add to the process, other than delays and costs, given that a clinical decision to admit has already been taken?
The On Call Director could be the £120k+ p.a. Finance Director, Daryll Chapman, a public sector accountant with no professional mental health qualifications.
Alternatively, it could be the new £120k+ Deputy Chief Executive of NSFT who doesn’t work for NSFT and whose LinkenIn says he lives in Kent, Mason Fitzgerald, who spent a staggering seven years accumulating two bachelors degrees in commerce and law and a masters degree in international business from not exactly top-rated academic institutions. Fitzgerald has subsequently added a risk management diploma, a Foundation Certificate in HR and a qualification for company secretaries. Mason Fitzgerald doesn’t work in commerce, the law, international business, HR, risk management or as a company secretary at NSFT. The only qualification Mason Fitzgerald seems to lack is in the area that would be most useful to him when making decisions about out of area beds: professional mental health. At least his massive ELFT salary will help him pay off his eternal student debts.
While whether ‘there are time limits to admit a SU’ influences the process, the physical and mental health needs of the patient do not. Patients are transported across the country by NSFT like low-value parcels or sometimes like wild animals in cages in vans without windows. There is no mention of medical examinations, risk assessments or support networks in this process. More care is taken by suppliers shipping seafood from Billingsgate or flowers from Holland. SU might as well stand for Shipping Unit as Service User. All we need to do is remember how Peggy Copeman or Neil Jewell died.
NSFT needs more front line staff, more local NHS beds and far fewer bureaucrats.
A clinically-led trust with decent values would not look like this.